Palliative Care, Pain Control, & End-of-Life Care
-
Background/Cultural Points:
Section titled “Background/Cultural Points:”Good pain control, end-of-life, and palliative care is generally deficient in Cambodia, as in many poorer countries, as is access to opioids. MMC patients with cancers, end-stage liver disease, and other conditions may be prescribed palliative/comfort care and family members may return to MMC for refills if the patient is too unwell to travel. This approach also avoids risking end-of-life patients dying in Phnom Penh away from home, which, due to cultural-religious issues, can be extra disturbing to many Cambodians. Hospice care may be available at NLF’s “Healing Home” in Phnom Penh.
-
Common Pain Management & Other
Section titled “Common Pain Management & Other”
- Give only one drug from the opioid and non-opioid group at a time
-
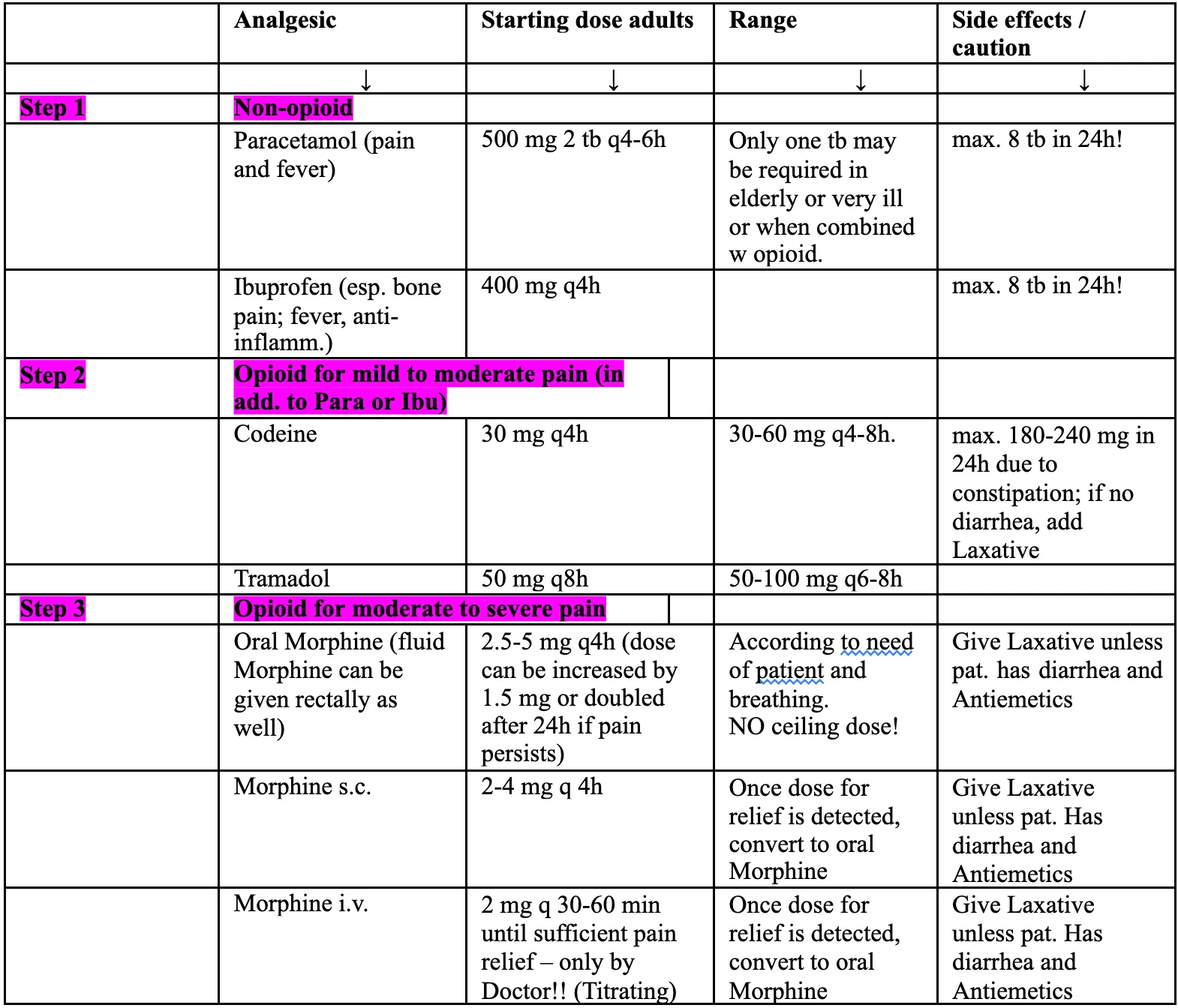
WHO Analgesic Ladder adaptation for MMC:
Section titled “WHO Analgesic Ladder adaptation for MMC:”- Step 1: Paracetamol (Acetaminophen) or NSAIDs (Ibuprofen is preferred, with 200 and 400mg tabs available)
- Step 2: Higher dose NSAID or Para+Codeine
- Step 3: Tramadol (Morphine Sulfate in exceptional situations)
-
Opioids are limited:
Section titled “Opioids are limited:”- Paracetamol + Codeine is available in two quantities: 500mg Para with 8mg Codeine or 500mg Para with 30mg Codeine. 500/8 is significantly cheaper than 500/30.
- No oral opioids are otherwise available (hydrocodone, oxycodone, etc)
- Morphine IM/IV may be available in limited quantity for use in OPD/IPD, but not for prescription/at-home use.
- Tramadol is preferred due to easy access (caution seizure d/o): 100mg twice daily to q6hr (max 400mg/day).
- Remember to prescribe stool softener and/or laxative with opioid prescription
-
Other medications:
Section titled “Other medications:”- Amytriptyline – Low dose (25-50mg qHS) has good benefit in Cambodia for neurogenic pain, anxiety, and sleep disorders; higher doses (or Fluoxetine) can be used for major depression
- Diazepam – 2.5-5mg qHS or q4-6hr can help in palliative care for sleep
- Prednisone – Excellent adjunct in certain pain/inflammation control situations, such as oropharyngeal cancer with secretions/obstruction, GI tract cancers; consider adjunct PPI (omeprazole) and Calcium+Vit D for long term use
- Docusate – 100mg stool softener (must be imported)
- Bisacodyl – 5mg laxative (cheapest option; readily available)
- Ensure/Nutrimama – consider nutritional/caloric supplementation as indicated; 1 large can is 10USD (patient must pay unless sponsor agrees to pay)
-
In Cambodia, as in many Asian contexts, families are often reluctant to tell their loved one a “bad news” diagnosis, believing that knowledge of the diagnosis will precipitate depression and death. At MMC, we typically break bad news to a close family member first, then explain that it is usually best to tell a patient his/her diagnosis to help him/her prepare for death, and that this knowledge will not cause the disease to progress quicker.
Sharing a “Bad News” Diagnosis:
Section titled “Sharing a “Bad News” Diagnosis:” -
Follow-Up:
Section titled “Follow-Up:”- Palliative meds are often many in number and type; 1 month follow up is best to ensure they are optimized.
- Ask the family in advance to inform MMC and bring back unused medications if their loved one passes away, if it’s not too inconvenient.
- If a patient dies at MMC, arrange for ambulance to transport back to home (transport of a deceased person is expensive; discuss with sponsor). A death certificate should also be written in English on MMC letterhead (time/date and cause of death).